Alignment of PAHO-WHO Planning and Budget Frameworks

Background and introduction
Created in 1902, within the Pan American Union (subsequently the Organization of American States), PAHO achieved independent status in 1924 and is the specialized health agency of the Inter-American System, in accordance with the provisions of the Charter of the Organization of American States. WHO Constitution was signed in 1946 and entered into force in 1948. In 1949, PAHO and WHO signed an agreement that recognizes PAHO as both an independent entity and as the WHO Regional Office for the Americas. Thus, PAHO retains a legal personality that is separate from WHO, has its own governance structure, and has a quota system based on the assessed scale adopted by the Organization of American States. PAHO also has its own strategic plan and programme budget, and accountability system, including monitoring, assessment and statutory reporting.
Within this context, and while upholding its status as an independent organization, PAHO, in its capacity as the WHO Regional Office for the Americas, works closely with WHO to implement global commitments approved by Member States, including those set out in the General Programme of Work and its associated Programme budgets. In its capacity as one of six Regions within WHO, the Regional Office for the Americas is known under the acronym AMRO. The Secretariat of PAHO is the Pan American Sanitary Bureau (PASB).
This document details the alignment between PAHO and WHO planning and budget frameworks. PAHO, as WHO, uses a results-based management approach to planning, budgeting, monitoring, assessment, and reporting. Alignment between PAHO and WHO frameworks is critical to facilitate effective planning, budgeting, monitoring, assessment, and reporting. This alignment makes it possible for PAHO to meet its obligations as AMRO, while responding to regional and country priorities.
Alignment happens in practice at all levels: from the alignment of strategic plans and results frameworks to the alignment of outcomes prioritized by Member States, which guide both PAHO and WHO Programme budget, as well as operational plans. Notwithstanding variances in the details of results elements, governance mechanisms, processes, and timelines, every effort is made to avoid duplication and ensure efficiency, accountability, and transparency at all levels of PAHO and WHO. The various frameworks and processes are outlined below.
Strategic plans and Results frameworks
The PAHO Strategic Plan 2020-2025 (SP20-25) outlines how the Organization contributes to the Sustainable Development Goals and the 13th General Programme of Work (GPW 13) Results Framework, as well as the Sustainable Health Agenda for the Americas 2018-2030 (SHAA2030), which is the health sector response in the Americas to the 2030 Agenda.
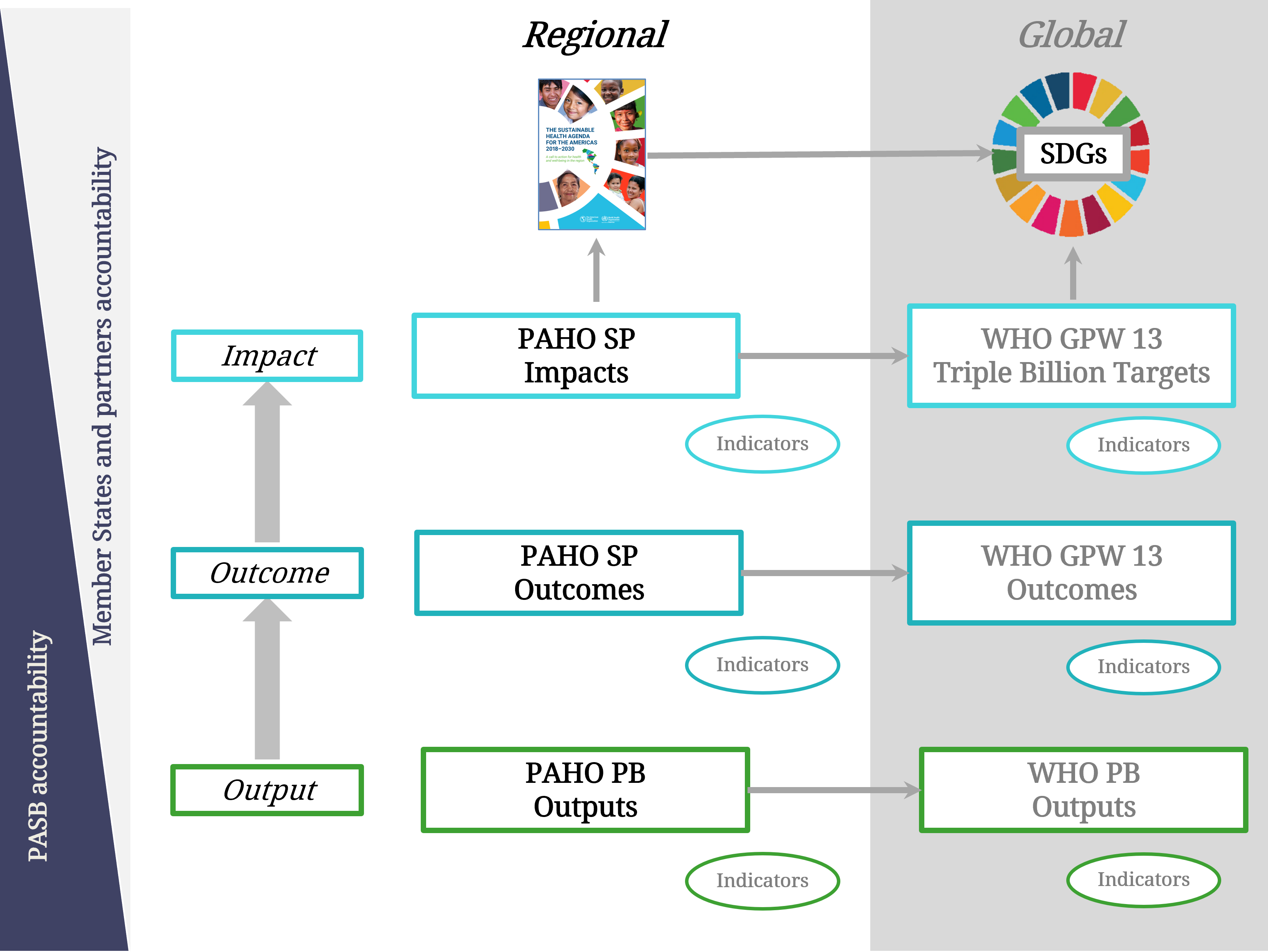
Figure 1 shows how the results in the PAHO Strategic Plan and Program Budget relate to the results and indicators in the WHO GPW 13 and Programme Budget, from output to impact level. As stated in the SP20-25, “[t]he regional elements have been designed to allow for accountability and reporting to the global level (consistent with PAHO’s function as the WHO Regional Office for the Americas) and to reflect regional needs and specificities in health.” Annex B of the SP20-25 contains a detailed crosswalk between the PAHO impact and outcome indicators and the GPW 13 programmatic indicators, as well as the SDG indicators and SHAA2030 targets.
Figure 1. PAHO and WHO Results Chain Alignment
Programme budget alignment
The total proposed PAHO Program Budget for 2024-2025 is $700 million for base programs1. For the 2024-2025 biennium, the proposed WHO Programme budget allocation to the Region of the Americas for base programs is $295.6 million.2 This allocation constitutes an important and integral part of PAHO’s total budget, representing 42% of the overall PAHO budget for base programmes.
To finance its approved budget, PAHO receives funding through assessed contributions from its Member States, allocations from WHO including WHO assessed contributions, and voluntary contributions from governments, international organizations, and private and public sector organizations. Due to the distinct nature of PAHO and WHO, and the arrangements between PAHO and WHO outlined above, the WHO allocation to the Americas, is considered to be financed only by funds originated and mobilized by WHO.
In practice, PAHO’s Programme budget financing is managed in an integrated manner along with the WHO’s approved budget for the Americas: no real separation occurs for the management of funds. Nevertheless, only financial resources originated and/or mobilized by WHO are reported back to WHO monitoring and reporting systems. This implies that WHO systems will show amounts of financing that do not represent the full amount of resources mobilized and implemented by PAHO to achieve the global joint objectives established and committed to by WHO Member States.
Table 1 shows the expected financing of PAHO base programs in the PB 2425 included in the draft PAHO Program Budget considered by Member States3, as well as the share of each financing source with respect to the total of the Base Programs.
Table 1. Proposed PAHO Program Budget 2024-2025 by Financing Source
Base Programs Only (US$)
| Source of financing | 2024-2025 | Share |
| PAHO net assessed contributions | 194,400,000 | 27.8% |
| PAHO budgeted miscellaneous revenue | 14,000,000 | 2.0% |
| PAHO voluntary contributions and other sources | 196,000,000 | 28.0% |
| WHO allocation to the Americas | 295,600,000 | 42.2% |
| TOTAL | 700,000,000 | 100% |
Alignment during Programme budget development process
PAHO’s integrated budget responds to country, regional and global priorities. The programmatic results structure upon which the programmatic prioritization process is performed ensures that priorities established by Member States for the PAHO Program Budget also serve the WHO Programme Budget, guaranteeing that there is alignment between what Member States prioritize for both Programme Budgets.
The prioritization process, which follows a consultative process with the national authorities, utilizes the PAHO-adapted Hanlon methodology approved by the PAHO 55th Directing Council (CD55.R2) to prioritize outcomes of the PAHO Strategic Plan. Country teams are advised to start the consultation process with a common understanding of the health situation of the country and PAHO/WHO’s technical cooperation.
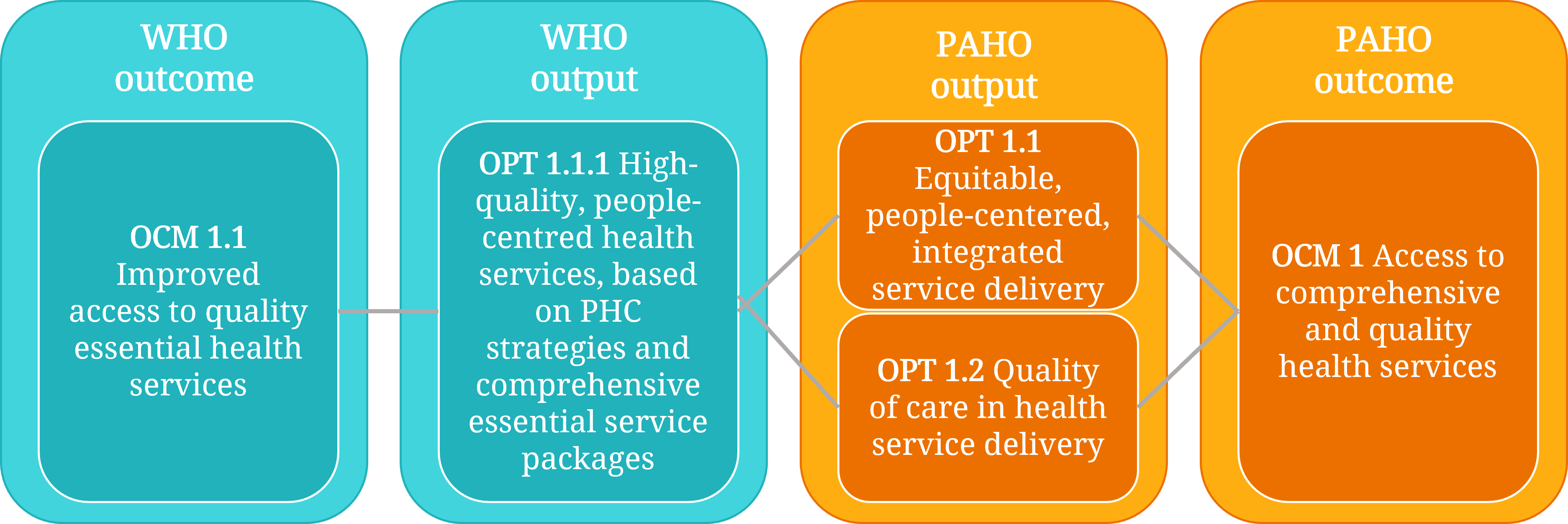
Respecting the commitment to Member States that they would complete the prioritization exercise only once for both the PAHO and WHO Programme budgets, once available, the priorities for the PAHO Program Budget from each country were translated into the WHO outcomes and outputs using a standardized approach, considering the PAHO-WHO outcome and output crosswalk (Figure 2). This crosswalk is critical not only for the alignment during the Programme budget development, but also for planning, implementation, monitoring, and reporting.
Figure 2. WHO – PAHO Output Crosswalk
Alignment during Programme budget implementation
Underpinning the implementation of the PAHO and WHO Programme Budgets, PASB regularly engages in strategic collaboration with WHO, participating in many high-level exchanges on strategic, technical, and operational matters, to represent the Region and identify priority areas for collaboration with WHO. PASB staff also participate in technical networks responsible for the planning, implementation, monitoring, and assessment of results of the GPW 13.4
Through such mechanisms, the Region influences key decisions at the policy level, contributes to governance and strategic frameworks, and advocates for greater support from WHO, including financing and strengthening of PAHO/WHO country offices. Information and knowledge sharing is critical for not only imparting the Region’s experience, but also for receiving knowledge that can foster improvements in the technical cooperation of PAHO with its Member States, including the adaptation of global norms and standards to the region. The importance of this collaboration was never more evident than during the response to COVID-19, in which PAHO both played a critical leadership role and participated actively in defining and implementing the global response efforts, both normative and operational.
The output crosswalk (Figure 2) ensures that each WHO output has one or more PAHO outputs for implementation of WHO Programme budget and related activities in the Region, while prohibiting scenarios where a given PAHO output is linked to more than one WHO output. Using the crosswalk between PAHO and WHO results, the priorities indicated by PAHO Member States are converted into the priorities according to the WHO results chain and implemented accordingly. Similarly, resource allocation and implementation of resources received from WHO is also performed and monitored, as applicable, utilizing this crosswalk to guarantee alignment across the two organizations.
Alignment during monitoring and reporting
Alignment of PAHO and WHO results frameworks is key for effective monitoring and reporting of the Region’s contribution to the results set out in the WHO GPW and PB. Results from the Region of the Americas are an integral part of the global midterm review and end-of-biennium results reports to the World Health Assembly. PAHO also presents an end-of-biennium results report to the Directing Council or Pan American Sanitary Conference, which also act as WHO Regional Committee for the Americas, for its full PAHO Program Budget.
PAHO has participated in the development, rollout, and refining of the WHO Output Scorecard methodology, as well as in the development of country success stories. These success stories highlight innovative and transformative practices and demonstrate the impact of PAHO and WHO at country level. These assessments are also opportunities for PAHO to share at the global level the Region of the Americas’ experience in results-based management, including in joint planning, monitoring, and assessment with Member States.
As for budget monitoring and implementation, both PAHO and WHO have developed PB portals, aligned with the International Aid Transparency Initiative (IATI), with the goal of increasing transparency and availability of information (PAHO PB Portal, WHO PB Portal). Budget implementation figures are published quarterly for PAHO and monthly for WHO. The WHO portal shows the corresponding figures for the AMRO portion of the PAHO PB and the PAHO portal shows the figures representing the totality of funding received by PAHO to implement the global and regional health priorities, benefiting all Member States of the Americas.