Founded in 1952, the Global Influenza Surveillance and Response System, or GISRS, is celebrating its 70th anniversary.
In the years leading up to GISRS’s founding, memories of the devastating impact of the great influenza pandemic in 1918, which led to as many as 50 million deaths, were still vividly present. The human influenza virus had been isolated in 1933, and the first vaccines had been licensed only a few years earlier in 1945 in the United States. GISRS was created to protect people against seasonal and pandemic influenza: a global problem needed a global solution. The image below shows a nurse taking a patient’s pulse in an influenza ward at Walter Reed Hospital, Washington, District of Columbia, in the United States of America.
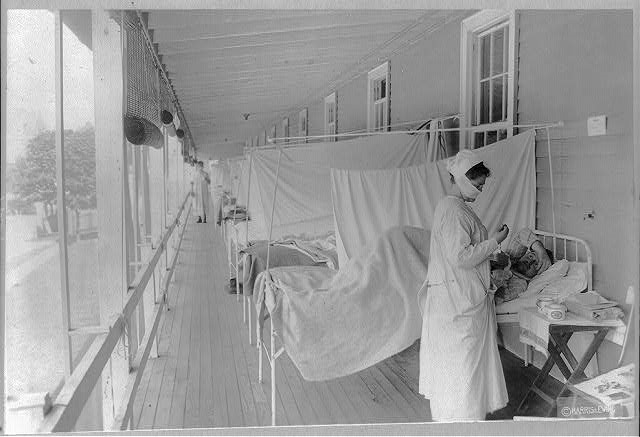
Library of Congress, Washington, D.C. (cph 3a39569)
1918
In 1952, only 25 countries had WHO-designated Influenza Centres in place and were able to report laboratory and epidemiological data to WHO, with other observer laboratories co-operating in various regions. The image below shows Professor J.D. Verlinde, from the Institute for Preventative Medicine at Leiden, Holland at his work-bench. The institute was one of the influenza centres collaborating with the World Influenza Centre in London.

1950
Laboratory investigations after influenza pandemics in 1957 and 1968 found that the novel pandemic viruses acquired 2 or 3 gene segments from an avian influenza virus and the remaining 5 or 6 segments from previously circulating human influenza A viruses. This finding shed light on the importance of influenza viruses circulating in animal reservoirs, particularly in aquatic fowl and pigs. The image below shows test-tube cultures in which respiratory viruses are grown. Samples were flown to the World Influenza Centre as soon as an outbreak of influenza occurred in any part of the world.

1968
During the 1960s and 1970s, the quality of influenza vaccines improved and their use increased predominantly in industrialized countries. WHO, based on the work by GISRS, began recommending viruses for inclusion in annual seasonal vaccines in 1973.
The GISRS network also continued to expand: by 1973, WHO had recognized 62 National Influenza Centres, of which 6 were in the African Region, 14 in the Region of the Americas, 2 in the Eastern Mediterranean Region, 30 in the European Region, 3 in the South-East Asian Region, and 7 in the Western Pacific Region.
The image below shows a nasal spray of live flu vaccine.
1976
New laboratory methods continued to be developed in the 1980s and 1990s. Molecular biology opened unforeseen opportunities to intensify the analysis and characterization of influenza viruses.
In late 2003 and in 2004, avian influenza A(H5N1) viruses caused human cases in connection with large outbreaks in poultry in several countries in Asia. The image below shows analysis being done in Indonesia.

2005
Between 2009 and 2010, a new A(H1N1) influenza virus emerged and led to a pandemic causing an estimated 100,000 to 400,000 deaths, with children and young adults most affected.
To improve pandemic influenza preparedness and response by improving and strengthening GISRS, an exemplary international instrument was unanimously adopted in 2011: the Pandemic influenza preparedness framework (PIP Framework). The PIP Framework supports the sharing of influenza viruses and the equitable and timely access to vaccines and other benefits.
Testing for antiviral resistance also became a routine task in GISRS laboratories, as it became clear that viruses had become resistant to some anti-influenza medications.
The image below shows the preparation of viral RNA (Ribonucleic Acid) samples by public health professionals at the Nepal Government laboratory for influenza diagnosis.

2010
As of January 2022, GISRS has grown to include 148 National Influenza Centres, seven WHO Collaborating Centres, four Essential Regulatory Laboratories, and 13 H5 Reference Laboratories. Between 2014 and 2019, GISRS tested an average of 3.4 million specimens every year. This surged to 6.7 million tests annually for influenza and 44.2 million tests for SARS-CoV-2 in 2020 and 2021. GISRS shares around 20 000 influenza virus samples every year to WHO Collaborating Centres, updates the weekly influenza situation based on laboratory and disease surveillance in the WHO FluNet and FluID systems directly or via regional platforms, and distributes timely risk assessments and alerts to countries.
Although GISRS was built to address influenza, it also serves as a critical resource for countries handling non-influenza emergencies. In the COVID-19 pandemic, GISRS has made significant contributions from the start. For example, GISAID, a long-term partner of GISRS, published the first SARS-CoV-2 sequence data hours after it became available. In many countries, National Influenza Centres of GISRS readily became primary hubs for national COVID-19 testing and response. Importantly, GISRS has been conducting integrated sentinel surveillance of influenza and SARS-CoV-2 to guide public health response to the two public health problems concurrently.
The image below shows a lab worker at Ethiopia’s National Influenza and Arbovirus Laboratory, testing for COVID-19 in February 2020.
2020