Global Programme to Eliminate Lymphatic Filariasis
In 1997, as a result of advances in the diagnosis and treatment of lymphatic filariasis (LF), the disease was classed as one of six infectious diseases considered to be “eradicable” or “potentially eradicable”. Consequently, the World Health Assembly adopted Resolution WHA 50.29, calling for elimination of the disease as a global public health problem. In response to this call, WHO launched the Global Programme to Eliminate Lymphatic Filariasis (GPELF) in 2000.
This resolution is further supported in WHA66.12 calling on the concerted efforts expand and implement interventions against neglected tropical diseases to achieve targets set out in the NTD Roadmap and sustain commitments noted in the London Declaration on Neglected Tropical Diseases.
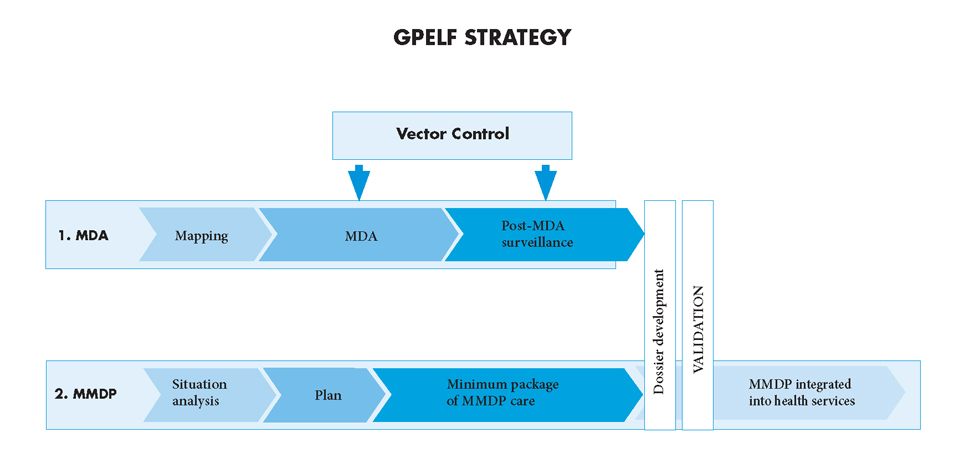
The elimination strategy has two components: (1) to stop the spread of infection (interrupting transmission); and (2) to alleviate the suffering of affected populations (controlling morbidity).
In order to interrupt transmission, districts in which lymphatic filariasis is endemic must be mapped and community-wide mass treatment programmes implemented to treat the entire at-risk population. Most of these programmes are based on once-yearly administration of single doses of two drugs given together. The following recommended drug regimens need to be administered once a year for at least 5 years, with a coverage of at least 65% of the total at-risk population:
1. Stop the spread of infection – MDA
In order to interrupt transmission, districts in which lymphatic filariasis is endemic must be mapped and a strategy of preventive chemotherapy called mass drug administration (MDA) implemented to treat the entire at-risk population. The following drug regimens are recommended for use in annual MDA for at least 5 years with a coverage of at least 65% of the total at-risk population:
- 6 mg/kg of body weight diethylcarbamazine citrate (DEC) + 400 mg albendazole; or
- 150 µg/kg of body weight ivermectin + 400 mg albendazole (in areas that are also endemic for onchocerciasis);
- 400 mg albendazole preferably twice per year (in areas that are also endemic for Loa loa).
An alternative and equally effective community-wide regimen in endemic regions is the use of common table salt or cooking salt fortified with DEC. DEC fortified salt has been used in only a few settings.
2. Alleviate suffering – MMDP
Successful MDA will prevent new infections and no new cases of clinical disease. To achieve the second aim of GPELF, a core strategy of morbidity management and disability prevention (MMDP) is needed. Suffering caused by the disease can be alleviated through a minimum recommended package of care to manage lymphedema and hydrocele. These services should be available within primary health care systems in all areas of known patients.

In 1997, the Fiftieth World Health Assembly adopted resolution WHA 50.29 on the elimination of lymphatic filariasis as a public health problem. Preliminary...

Managing morbidity and preventing disability in the Global Programme to Eliminate Lymphatic Filariasis...
In 1997, the World Health Assembly resolved to eliminate lymphatic filariasis as a public-health problem. In 2000, the World Health Organization (WHO)...

Integrated vector management to control malaria and lymphatic filariasis -- WHO position statement
The World Health Organization (WHO) promotes integrated vector management (IVM) to improve the cost effectiveness of vector-control operations, and to...
Progress
NTD Roadmap Target: Global Elimination as a Public Health Problem by 2020
Validation
A framework for the control, elimination and eradication of neglected tropical diseases (NTDs) has been developed which outlines a standardized process for reviewing and confirming the achievement of NTD roadmap targets. A process of validation will be used for formal confirmation of elimination as a public health problem. Countries wishing to be recognized for their success can make a request to WHO for such acknowledgement with adequate evidence that elimination targets have been achieved. The minimal information necessary for a dossier includes: (i) a description and supporting data of classification of endemicity for each implementation unit (IU); (ii) results of mass drug administration (MDA) and other interventions implemented; (iii) monitoring data on the interventions; (iv) epidemiological data from sentinel and spot-check sites; (v) results from Transmission Assessment Survey (TAS) prior to stopping MDA and subsequent TAS during post-MDA surveillance; (vi) data supporting availability and provision of the basic recommended package of care for lymphatic filariasis patients.
Milestones towards validation
- Stop the spread of infection through mass drug administration
- Implement MDA in all endemic areas (100% geographical coverage)
- Reduce infection below a threshold at which transmission is not sustainable in all endemic areas and stop MDA
- Demonstrate sustained reduction of infection below the threshold no earlier than 4 years after stopping MDA
- Alleviate suffering by managing morbidity and preventing disability (MMDP)
- Define burden of disease (estimates of the number of patients)
- Recommended minimum package of care available in all areas of known patients (100% geographical coverage)
Where do we stand
China and the Republic of Korea were declared to have eliminated lymphatic filariasis as a public health problem in 2007 and 2008, respectively. Of 73 countries listed by WHO as being endemic for lymphatic filariasis, 18 countries have completed interventions and are conducting surveillance to validate elimination. An additional 22 countries had delivered MDA in all endemic areas and are also on track to achieve elimination. The remaining 33 countries have not been able to achieve 100% geographical coverage; 10 of these have yet to initiate preventive chemotherapy or submit evidence that MDA is not required.
Mass treatment is ongoing in 45 countries. Ten countries have not started treatment or submitted evidence indicating treatment is not required.